Journal of Ovarian Research A responsividade do folículo antral avaliada por RaTe de saída folicular
https://doi.org/10.1186/s13048-019-0522-4 | 18 de Outubro de 2019
Abstract
Background: The antral follicle count is a marker of ovarian reserve. Follicular Output RaTe (FORT) evaluates the proportion of follicles responsive to exogenous follicle stimulating hormone (FSH) during controlled ovarian stimulation. Our objective was to evaluate whether the diameter (AFC6: ≤ 6 mm or AFC > 6: > 6 mm) of the follicular cohort could be a predictor for ovarian responsiveness, assessed by FORT, in a prospective cohort with 92 women with IVF indication, regular cycles and no abnormality in both ovaries.
Results: The mean age (±SD) of the women was 36.03 years (± 3.87 years), the median FORT was 43.30%. We found correlation between the FORT and AFC6 (r = − 0.237, P 0.023) but not between the FORT and AFC > 6 (r = − 0.055, P 0. 602).
Conclusions: The inverse correlation between FORT and AFC6 suggests that those follicles were less responsive to the exogenous FSH.
Keywords: Follicular output rate, FORT, Controlled ovarian hyperstimulation, Antral follicle size, Ovarian responsiveness
Background
Follicular recruitment and development in response to controlled ovarian hyperstimulation (COH) with gonad- otropins are essential in the treatment of infertility with assisted reproductive techniques [1]. The prediction of this ovarian response, which is evaluated through the ovarian reserve, is fundamental for both prognosis and treatment individualization.
Treatment individualization entails selecting the best GnRH analogue protocol and the best initial gonado- tropin dose to achieve the ideal ovarian response be- cause both low and hyper-responses are known to potentially lead to cycle cancellation and increased costs [2]. While a low ovarian response may decrease the chance of pregnancy, an exaggerated response presents the risk for the development of ovarian hyperstimulation syndrome [3–5].
Ovarian reserve has complex mechanisms that can be influenced by age, genetics and environmental factors [6]. Several markers of ovarian reserve have been stud- ied in the last few decades, but an ideal marker still has not been established. Response prediction through ovarian reserve testing is superior to that through chronological age alone. The antral follicle count (AFC) and anti-Müllerian hormone (AMH) are currently con- sidered to have the best sensitivity and specificity to predict the ovarian response, despite them having 10– 20% false-positive rates [7]. Since ovarian responsive- ness seems to be influenced by many factors, nomo- grams, based mostly on the age and AMH, AFC and day 3 FSH levels of women, were developed in the past few years to determine the individualized FSH starting dose in IVF cycles to reduce costs and improve the chances of pregnancy [8, 9].
Ovarian responsiveness is one of the most com- monly studied parameters in clinical research con- cerning IVF treatment [10]. Traditionally, the number of oocytes retrieved is the main outcome measure of ovarian responsiveness to gonadotropin stimulation [5]. However, the number of pre-ovulatory follicles ob- tained at the end of COH is not a reliable reflection of the antral follicle sensitivity to FSH, and it is strongly corre- lated with the number of antral follicles before ovarian stimulation [11]. Although, maybe not only the number of antral follicles, but also their size, is important. The Fol- licular Output RaTe (FORT) evaluates the proportion of follicles that were responsive to FSH and is calculated by dividing the number of preovulatory follicles (16–20 mm) × 100 by the antral follicle count (3–8 mm), and it is known to be correlated to the outcomes of IVF, including pregnancy rates [12].
The distinction of various size categories may be rele- vant since several studies show that the endocrine func- tion of a follicle is related to its diameter. [13, 14]. A previous study reported that pregnant patients had the highest numbers of antral follicles between 5 and 10 mm. [15]. Another study demonstrated that the number of follicles of 2–6mm declines with age but that the number of follicles of 7–10 mm remains stable, suggest- ing that follicles smaller than 6 mm may represent the functional capacity of the ovary [14]. Mechanisms of the sensitivity of antral follicles to FSH remain to be com- pletely elucidated. However, an adequate responsiveness to FSH is a characteristic of healthy and differentiated granulosa cells [16, 17].
The main objective of this study was to evaluate whether the pool of follicles up to 6 mm or larger than 6 mm correlates better with the ovarian response to the controlled stimulus, evaluated through the FORT.
The secondary objectives of this study were to evaluate the correlation among the FORT and other factors that can influence ovarian responsiveness, such as age, body mass index (BMI), and the levels of AMH and FSH.
Materials and methods
Subjects
We prospectively studied 92 patients, ranging from 26 to 45years of age, who underwent COH for IVF+embryo transfer (ET) from January 2015 to August 2017. All of the patients met the following inclusion criteria: 1) both ovaries were present, morphological abnormalities (such as cysts, endometriomas, etc.) were absent, and transvagi- nal ultrasound scans having adequate visualization; 2) regular menstrual cycles lasting between 25 and 35 days. The exclusion criteria were: 1) current or past diseases af- fecting the ovaries or those affecting the secretion, clear- ance, or excretion of gonadotropin or sex steroids; 2) clinical and/or biological signs of hyperandrogenism; 3) diagnosis of polycystic ovarian syndrome.
Local institutional review board approvals for the use of clinical data for research studies were obtained and written informed consent was obtained from all patients.
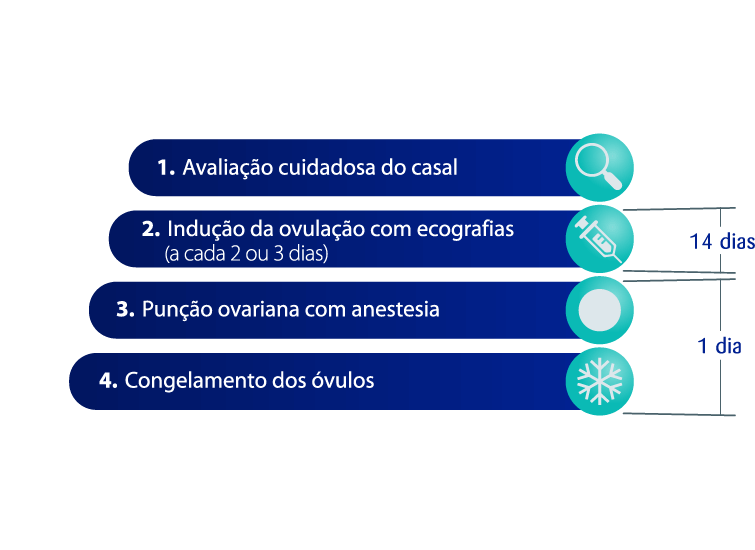
COH and IVF-ET protocol
Patients were submitted to COH with a flexible GnRH antagonist protocol [18]. In brief, between day 1 and day 3 of the menstrual cycle, the gonadotropin, either Elonva® 100 mcg or 150 mcg (Alfacorifolitropina, Merck & Co), was administered. The choice of the gonado- tropin dose was decided based on patient’s weight: 100 mcg was selected for patients weighing less than 60 kg, and 150 mcg was selected for patients weighing 60 kg or more. According to the follicular response and after the seventh day of the COH, Menopur® (human menotropin gonadotropin, hMG, Ferring) was used if necessary (75– 300 IU). Orgalutran® 0,25 mg (GnRH antagonist, Scher- ing Plough) was started when a follicle reached 12 mm. Choriomon® 5000 IU (Human chorionic gonadotropin, hCG, Meizler) was administered as soon as ≥2 preovula- tory follicles (16–22mm in diameter) were observed. Oocytes were retrieved by transvaginal ultrasound- guided aspiration 36 h after hCG administration. The lu- teal phase was supported with 600mg/day micronized progesterone administered continuously by the vaginal route, starting on the evening of the embryo transfer. The embryo(s) transfer was performed on day 2, 3 or 5, depending on embryo development. Clinical pregnancy was defined as the presence of an intrauterine embryo with cardiac activity at around 6 weeks after treatment.
FORT calculation
The calculation of the FORT is also explained elsewhere [12]. The FORT was calculated by using the ratio be- tween the number of preovulatory follicles (PFC) on hCG day × 100 and the number of AFC at baseline. The choice of considering only the 16–22mm follicles for the calculation of the FORT was determined in a previ- ous investigation by our group [13] and represented a methodological attempt for discriminating the follicles that were the most FSH-responsive among the cohort of small antral follicles.
Hormonal measurements
Blood was collected by venipuncture on day 1–3 of a pre- ceding cycle (1–3months prior to the IVF procedure). Serum AMH levels were determined using an ultrasensitive enzyme-linked immunosorbent assay (Beckman Coulter, Inc., Brea, CA, USA), with sensitivity < 0.02–18.4 ng/mL and the maximum intra- and inter- assay imprecision (CV) were 12 and 14%, respectively.
Serum FSH levels were determined using a chemilumin- escence immunoassay (Siemens Om-MA Immulite 2000, Munich, Germany). The range of detection of the im- munoassay were 0.3–200 IU/L, and intra-and inter-assay CVs were 3 and 5%, respectively.
Ultrasound measures
The antral follicular size and count assessments were performed with a 5–6 MHz transvaginal probe Famio 5 (Toshiba, Japan) prior to gonadotropin administration on menstrual days 1–3. The antral follicle count was de- fined as the number of follicles with a diameter of 3–8 mm. The follicular size was given as the mean of the two largest diameters in the same plane and perpendicu- lar to each other. In this paper, our baseline AFC count was divided into follicles with a diameter of 6 mm or less and those with a diameter greater than 6 mm. The folli- cles with a diameter of 6 mm or less are represented by AFC6, and the follicles with a diameter larger than 6 mm and up to 8 mm were represented by AFC > 6.
Statistics
The measure of central tendency used for parametric data was the mean, and the measure of variability used was the standard deviation (SD). The median and the minimum and maximum values were used when nor- mality could not be ascertained. The Gaussian distribu- tion was assessed by the Shapiro-Wilk test. Moreover, we performed a multivariable analysis considering FORT as a dependent variable and AFC, AFC6, AFC > 6, AMH, BMI, FSH and age as independent variables. The rela- tionship between two continuous variables was assessed by a correlation analysis when they were independent from each other and by regression when there was a dependent relationship between the variables. Spear- man’s test was used to determine if the correlation coef- ficients (r) were significantly different from zero. Considering a correlation coefficient of >0.3 and a power of 80%, the sample size calculation was 85 pa- tients. A value of P < 0.05 was considered statistically sig- nificant. The data were analyzed with SPSS 18.0 [SPSS Inc., released 2009, PASW Statistics for Windows, ver- sion 18.0, Chicago].
Results
The study population consisted of 92 women. The char- acteristics and reproductive outcomes of the patients are shown in Table 1. At the time of inclusion, the age of the women was 36.03 ± 3.87 years (mean ± SD). At base- line, the AFC median was 8.50 follicles (range: 2–25 fol- licles), AFC6 median was 6.00 follicles (range: 0–25 follicles) and AFC > 6 median was 1.00 follicles (range: 0–11 follicles). Overall, the median FORT was 43.30% (range: 6.67 – 100.00%). A median of 5.00 oocytes (range: 0–30 oocytes) were retrieved. The median AMH level was 1.69 ng/mL (range: 0.09–16.50 ng/mL), and the median FSH level was 6.95 IU/L (range: 1.50–12.50 IU/ L). The median BMI was 22.40kg/m2 (range: 19.00– 31.20 kg/m2).
Camila Bessow , Rafaela Donato , Tatiane de Souza , Rita Chapon , Vanessa Genro and
João Sabino Cunha-Filho1,2,3